By Dr Sumit Toor
Introduction
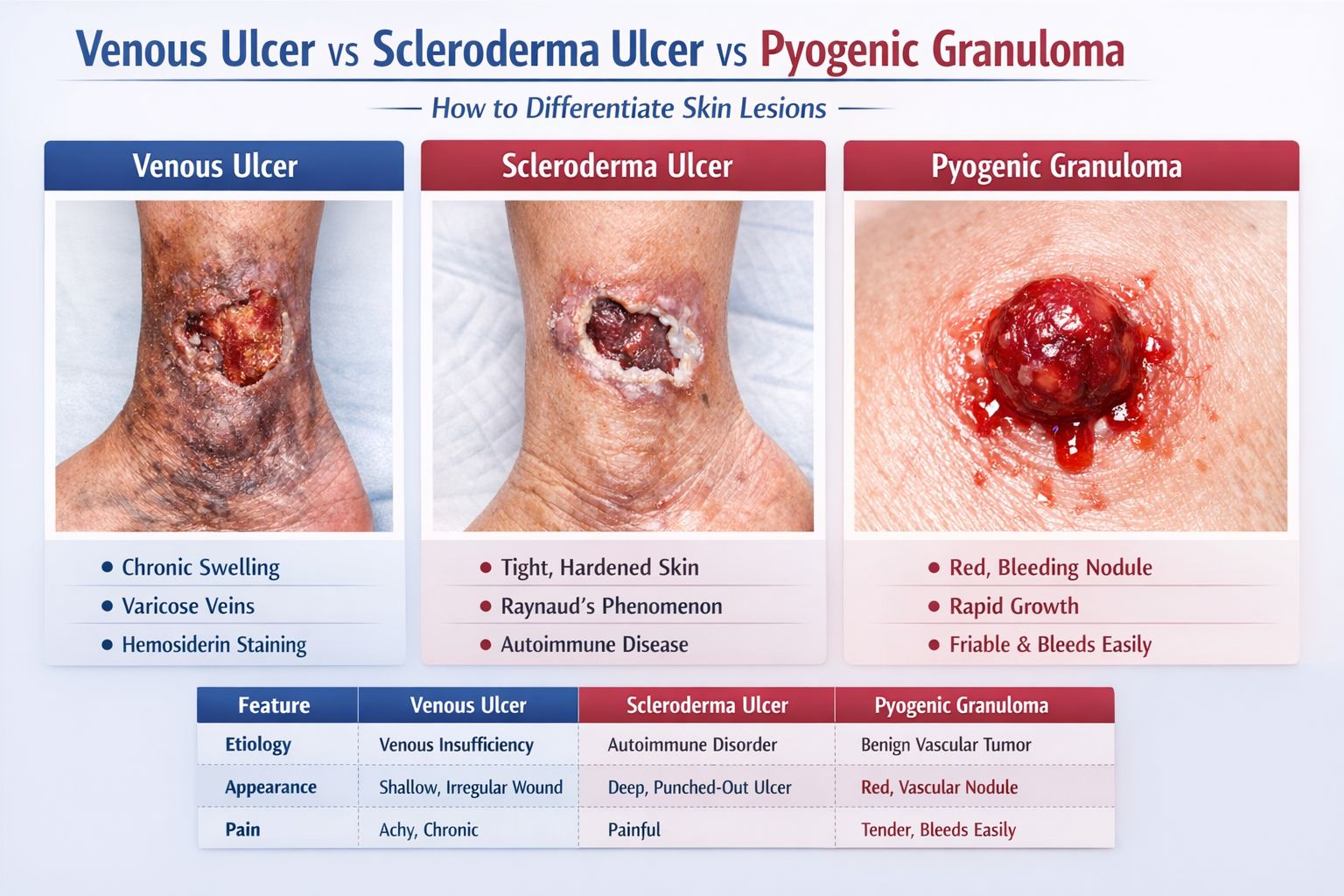
Identifying skin lesions on the lower extremities is a common challenge for both patients and clinicians. While many leg sores may appear similar at first glance, their underlying causes can range from chronic circulatory issues to complex autoimmune diseases or benign vascular growths. Distinguishing between Venous Ulcers, Scleroderma Ulcers, and Pyogenic Granulomas is critical because the treatment for one may be ineffective—or even harmful—for another.
Accurate diagnosis ensures that the root cause is addressed, preventing complications such as chronic infection, permanent scarring, or unnecessary surgical procedures. This guide explores the unique characteristics of these three conditions to help navigate the diagnostic process.
Venous Ulcers: The Result of Poor Circulation
Venous ulcers are the most common type of chronic leg wound, accounting for the majority of lower-extremity ulcerations. They are primarily caused by venous hypertension, which occurs when the valves in the leg veins fail to work correctly (valve incompetence). This leads to blood pooling in the lower legs, increasing pressure and eventually causing skin breakdown.
Typical Clinical Appearance and Location:
- Location: Usually found in the “gaiter area,” which is the region between the mid-calf and the medial malleolus (the inner ankle bone).
- Appearance: These ulcers are often shallow with irregular borders. The wound bed is typically ruddy or red, often covered with yellow fibrous tissue.
- Associated Signs: Patients often exhibit edema (swelling), varicose veins, and hemosiderin deposition (a brownish-orange staining of the skin). In chronic cases, the skin may become hard and woody, a condition known as lipodermatosclerosis.
Diagnostic Workup and Management:
Diagnosis is often confirmed via a venous duplex ultrasound to assess blood flow and valve function. Management focuses on reducing pressure through compression therapy (bandages or stockings), leg elevation, and specialized wound dressings. In some cases, minimally invasive procedures to treat the underlying varicose veins may be necessary.
Scleroderma Ulcers: An Autoimmune Challenge
Scleroderma, or systemic sclerosis, is an autoimmune condition characterized by the overproduction of collagen, leading to the hardening of the skin and internal organs. Ulcers in scleroderma patients are primarily the result of microvascular ischemia (lack of blood flow to small vessels) and sclerodermatous skin changes.
Typical Clinical Appearance and Location:
- Location: These ulcers frequently occur over bony prominences, such as the knuckles, elbows, or the tips of the toes and fingers (digital ulcers). However, they can also appear on the lower legs.
- Appearance: They are typically small, deep, and exquisitely painful. Unlike venous ulcers, they often have a “punched-out” look.
- Associated Systemic Findings: Patients may also experience Raynaud’s phenomenon (fingers turning white or blue in the cold), skin tightening (sclerodactyly), and telangiectasia (small dilated blood vessels).
Treatment Approach:
Management requires a multidisciplinary approach. Treatment often involves vasodilators to improve blood flow, pain management, and immunosuppressive therapies to address the underlying autoimmune activity.
Pyogenic Granuloma: The Rapidly Growing Mimic
A Pyogenic Granuloma is not actually an infection (pyogenic) nor a true granuloma; it is a lobular capillary hemangioma. It is a benign vascular growth that can appear suddenly and grow rapidly, often mimicking an ulcerative lesion or even a malignancy like melanoma.
Typical Morphology and Growth:
- Appearance: It usually presents as a bright red, friable (easily crumbled) nodule that may have a “collarette” of scale at the base.
- Bleeding Tendency: One of its most defining features is that it bleeds profusely with even minor trauma.
- Growth Pattern: It evolves over a few weeks, which can be alarming to patients.
Histopathology and Treatment:
Because it can look like more serious skin cancers, a biopsy is often performed. Once confirmed, treatment options include shave excision, cautery, or laser therapy to remove the lesion and prevent recurrence.
Comparative Table: Differentiating the Lesions
The following table provides a quick reference to distinguish between these three distinct conditions:
| Feature | Venous Ulcer | Scleroderma Ulcer | Pyogenic Granuloma |
|---|---|---|---|
| Etiology | Venous hypertension | Microvascular ischemia/Fibrosis | Vascular proliferation |
| Typical Age | Elderly/Middle-aged | 30–50 years (mostly women) | Children/Young adults/Pregnant women |
| Location | Inner ankle (Gaiter area) | Bony prominences/Fingertips | Hands, face, or lower legs |
| Appearance | Shallow, irregular borders | Small, deep, “punched-out” | Bright red, raised nodule |
| Pain | Mild to moderate | Severe | Usually painless (unless irritated) |
| Bleeding | Minimal | Minimal | Frequent and profuse |
| Systemic Signs | Varicose veins, edema | Raynaud’s, skin tightening | None |
| Treatment | Compression, wound care | Vasodilators, wound care | Excision, cautery |
Clinical Red Flags: When to Seek Urgent Care
While the conditions above are common, clinicians must always remain vigilant for clinical red flags that suggest a more serious underlying issue, such as malignancy (e.g., Squamous Cell Carcinoma or Amelanotic Melanoma). Suspect malignancy or mixed pathology if:
- The ulcer does not heal despite standard treatment for 3–6 months.
- The borders of the ulcer become rolled, everted, or excessively firm.
- There is a sudden change in the appearance or a rapid increase in size.
- The patient has a history of skin cancer in the area.
In these cases, a biopsy is mandatory to rule out skin cancer or rare inflammatory conditions like Pyoderma Gangrenosum.
Conclusion
Differentiating between venous ulcers, scleroderma ulcers, and pyogenic granulomas is essential for effective wound management. Because these lesions can overlap in appearance, a thorough evaluation by a dermatologist, plastic surgeon, or vascular specialist is highly recommended. By identifying the specific cause of a skin lesion, healthcare providers can implement a targeted treatment plan that promotes healing and improves the patient’s quality of life.